
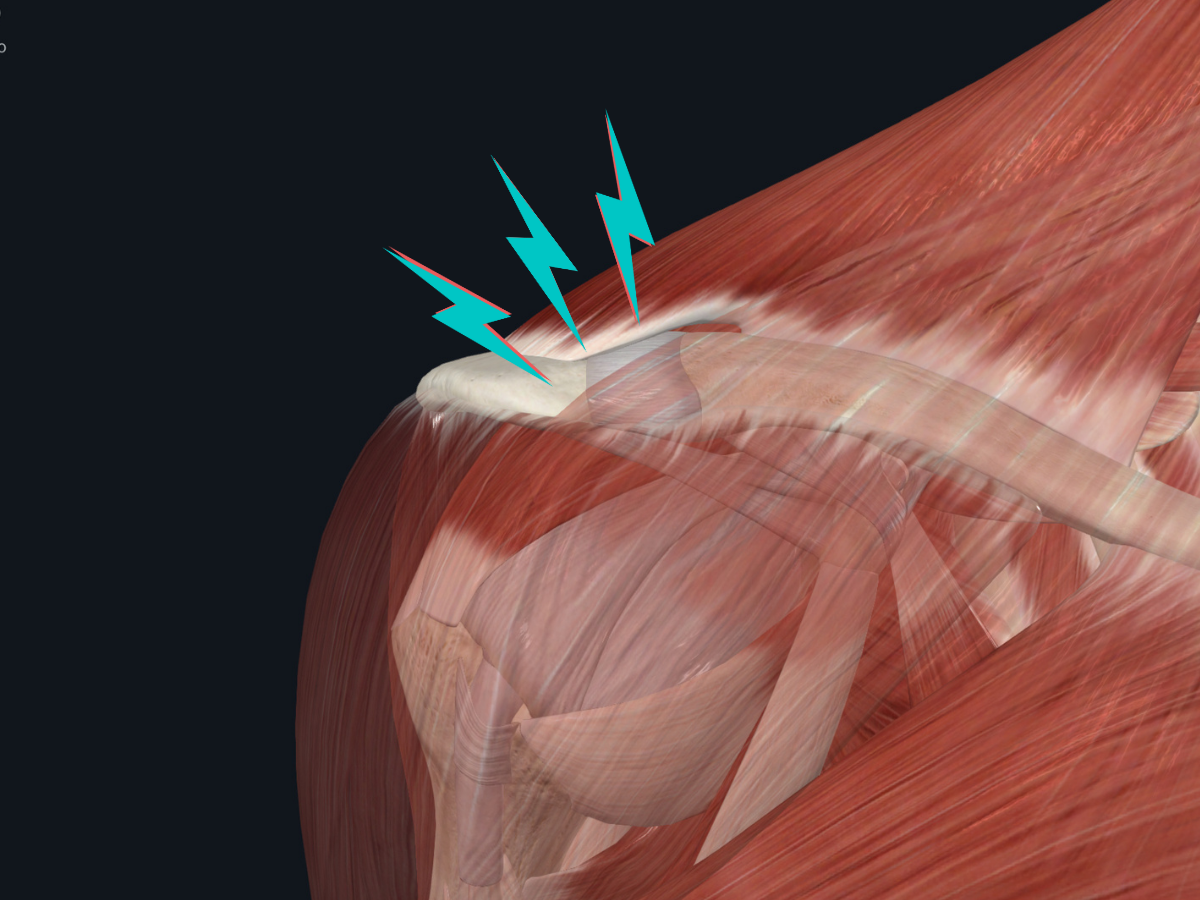
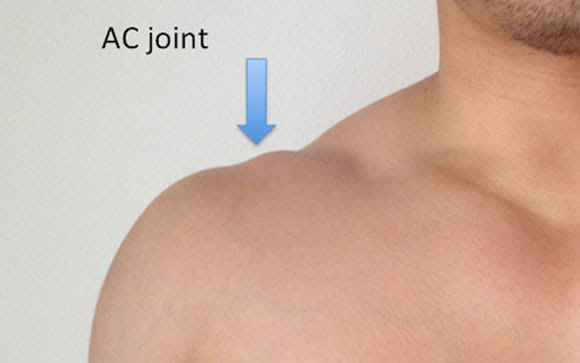
What is the acromioclavicular (AC) joint?
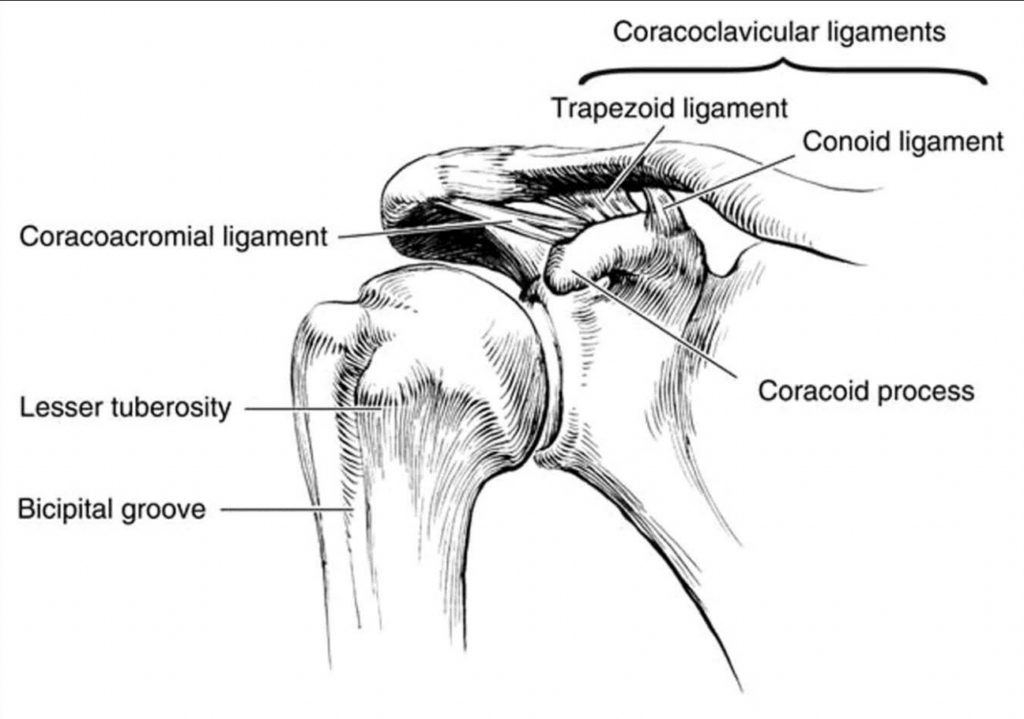
The acromioclavicular (AC) joint is a joint located at the top of the shoulder. It is formed by the clavicle (collarbone) and the acromion (a bony projection off the shoulder blade). This joint is responsible for a small amount of shoulder movement. The AC joint is held together by ligaments, which can be torn by a fall or other injury. It is stabilized by the capsule and associated ligaments, including the superior, inferior, anterior, and posterior AC ligaments, as well as the coracoclavicular (CC) ligaments. The AC ligaments are good at keeping the collarbone from moving backwards or rotating. The CC ligaments primarily help prevent upward and downward motion at the joint.
What are the types of injury to the AC joint?
The most common type of injury to the AC joint is a separation, also called a shoulder separation or a separated shoulder. This occurs when the ligaments that connect the clavicle to the shoulder blade are torn. AC joint injuries are usually the result of either direct or indirect trauma. This means that somebody either fell directly onto their shoulder, or they fell onto their hand while it was outstretched. People with this injury, oftentimes young athletes, often have a lot of pain in their shoulder and may have a deformity. There are different types of AC joint injuries, and depending on the type, treatment can be either surgical or nonsurgical.
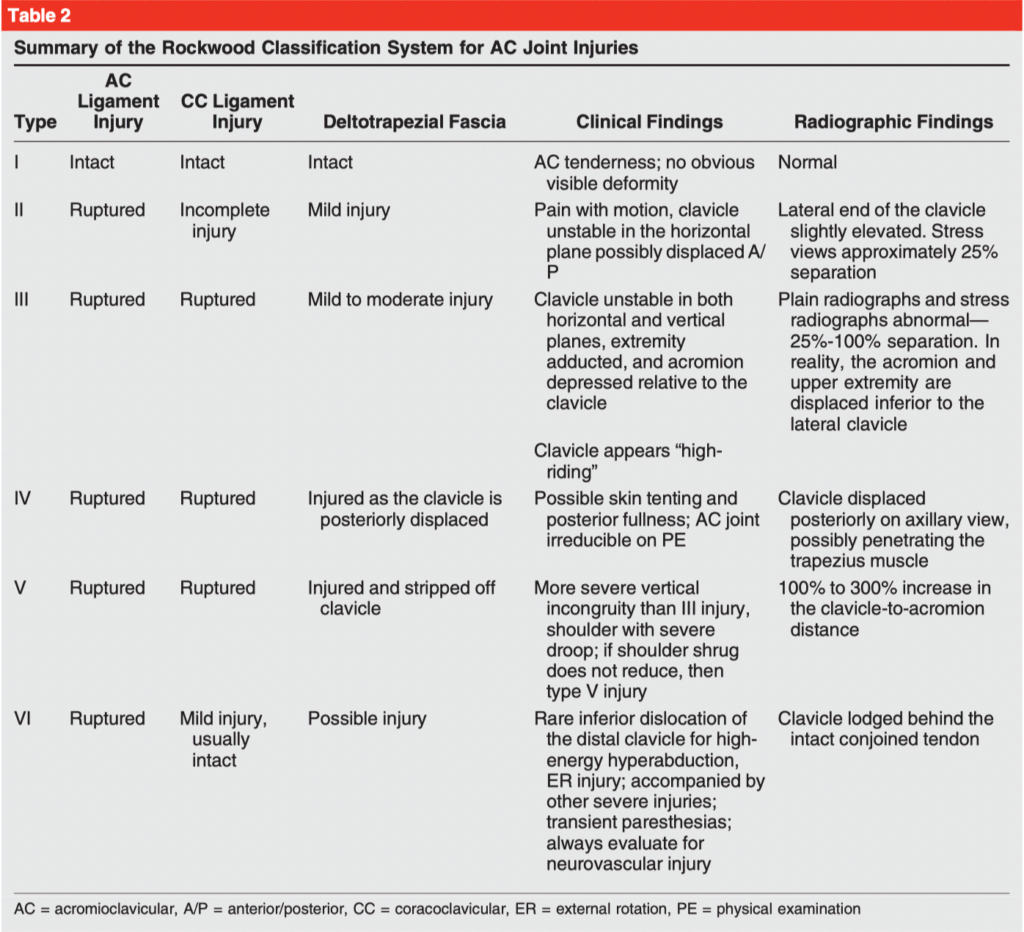
The Rockwood Classification system grades injuries to the AC and CC ligaments from III to VI, with III being the most severe. In 2014, the ISAKOS Upper Extremity Committee suggested subdividing grade III injuries into type IIIA (stable) and type IIIB (unstable).
How is an AC joint separation diagnosed?
The diagnosis of an AC joint separation is typically made based on a combination of the patient's symptoms and physical examination findings. Imaging studies, such as X-rays, may also be used to confirm the diagnosis.
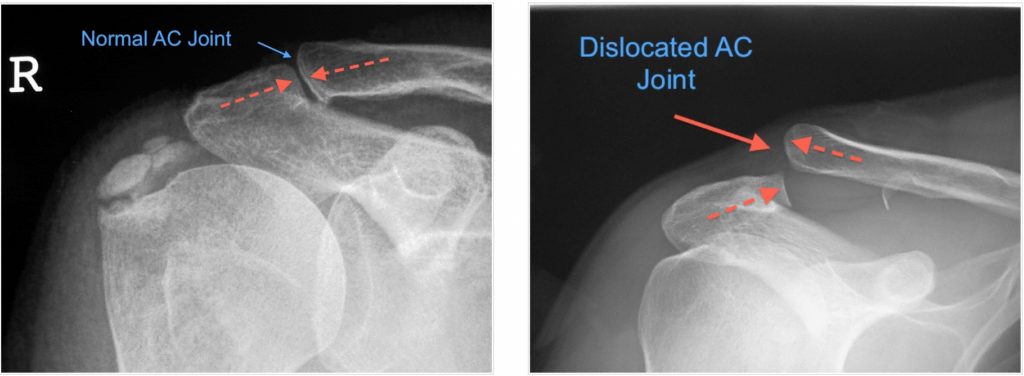
In some cases, MRI can be useful to evaluate for any additional intra- and/or extra-articular glenohumeral joint pathology. Other injuries associated with AC joint separation can be variable and include shoulder joint pathology in 15% to 50% of patients with high-grade AC joint separations.1
What are the signs and symptoms of an AC joint injury?
The signs and symptoms of an AC joint injury include pain and tenderness over the front of the shoulder, swelling, and bruising. The shoulder may be stiff, weak, difficult to move, and held in a position of partial flexion.
Do I need an AC joint brace?
A sling is worn in the early stages of recovery depending on the severity of the injury. Rigid taping of the AC joint can also help relieve symptoms, especially when transitioning away from the sling.

What is the treatment for AC joint pain?
Type I and II
Nonsurgical treatment is recommended for nearly all patients with type I and II AC joint injuries. This means that people with these injuries usually don't have to have surgery. Type I injuries can often be managed with immobilization in a simple sling for 1 to 3 weeks, whereas a longer course of sling immobilization may be necessary for type II injuries. Other nonsurgical treatment modalities include nonsteroidal anti-inflammatories, activity modification, physiotherapy, and cryotherapy. Physiotherapy can be initiated within the first 2 weeks to improve range of motion, after which time gentle strengthening exercises can be introduced. Contact sports and heavy lifting are typically avoided for 1 month, but return to full activities can take as long as 2 to 3 months.
Type III
The optimal management of type III AC joint injuries continues to be controversial. Although very few level I or II studies are available to guide clinical and surgical decision-making, multiple lower-level studies have been published favouring nonsurgical approaches. In addition, several studies on physician preferences for the management of these injuries have been published. Nonsurgical management of type III injuries uses the same approach as described previously for type I and II injuries, although the duration of sling immobilization is likely to be longer, approaching 3 to 4 weeks. In a series of 44 patients with type III AC joint injuries managed nonsurgically, the researchers noted good-to-excellent outcomes in all but one patient at 5 years after injury.
Types IV and V
Surgical intervention is recommended for patients with Rockwood type IV and VI injuries. For patients with type V injuries, many factors must be considered when deciding on surgical versus nonsurgical management, including the status of the surrounding skin and soft tissue, medical comorbidities, and expectations/goals of the patient, including any desire to return to contact sports.
Exercises for AC joint pain
Phase I
The early stages of rehabilitation involve protecting the joint to allow it to heal. This includes a period of immobilization in a sling as detailed above, depending on the type of AC joint injury. After this brief period, early mobility exercises can be performed in a “short-lever” position (i.e. with a bent arm) with the arms close to the body to minimize stress on the healing tissue. Once these movements are tolerated, progressions can include certain “long-lever” exercises in positions slightly away from the body. Little to no external resistance is recommended in this stage. Movements to avoid include shoulder shrugging, elevation, weight-bearing through the hands, and cross-body shoulder adduction.
Phase II
Resistance can be progressed in this stage, with light weights or resistance bands to start, and increasing as tolerated. Exercises can be progressed away from the body and include more dynamic movements, still with a focus on shoulder stability and control. The kinetic chain (i.e. other joints that are involved in shoulder function) can also be incorporated into the exercise program at this time.
Phase III
In the later stages, movements that stress the AC joint can be gradually re-introduced. These include weight-bearing exercises, overhead movements, and upper body plyometric drills. This phase focuses on restoring symmetrical strength and stability on the injured side while preparing the athlete to return to sports participation.
Overall, the vast majority of people with shoulder separation return to their activity, typically within 2-3 months depending on the severity of the injury.
References
- https://pubmed.ncbi.nlm.nih.gov/31008872/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8975563/
.png)