The Complete Guide to a Bone Stress Fracture
Humans are built to be able to run long distances because it…


In 2011, Nike unveiled the SPARQ Vapor Strobes eyewear. They were designed to improve cognitive processing, reaction time, attention, anticipation, and hand-eye coordination in athletes; but the history of stroboscopic visual training (SVT) goes back more than a decade earlier. This type of training was originally inspired by Michael Jordan – who was known to have trained using strobe lights to acclimate himself to photographer’s camera flashes while standing at the free throw line.1 The story goes that MJ noticed improvements in other aspects of his game – the strobe lights seemed to slow things down on the court. It was a training tool that was used by the best players at the time and kept secret from the competition. From nightclub strobe lights to early eyewear prototypes – such as the Strobe Spex – to Nike SPARQ and now Senaptec Quad Strobes, stroboscopic visual training has evolved from the early days and has seen a resurgence in popularity for athletic performance and a burgeoning interest in musculoskeletal injury rehabilitation.
Your brain integrates three main sensory systems to control your muscle output and help you navigate the world – vision, proprioception, and vestibular inputs. The vestibular system is your inner ear. It generates the sensation of moving up and down (in a roller coaster, boat or elevator) and helps orient your eyes with your head movements. The proprioceptive system is the kinaesthetic feedback from your body – touch, acceleration, positioning, orientation, and more. Single-leg balance relies on your brain detecting where your entire body is at all times in order to change how your muscles fire to keep you from falling over.
In normal tissue, sensory information comes from the receptors in the joint and is transmitted to the brain for further processing. The brain integrates this information, along with visual and vestibular inputs, and uses it to control your body as you move and react to your environment.
After an injury to a joint, such as an ACL tear in the knee, the sensory information from your proprioceptive system in the injured region is disrupted. This in turn affects your brain’s ability to get a clear picture of where your body (specifically your injured limb) is located in space.
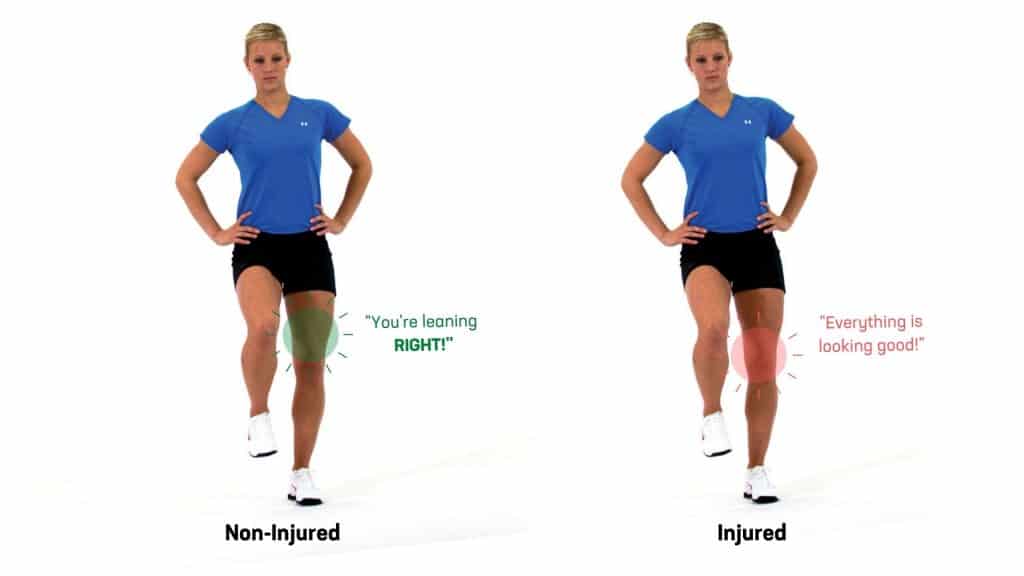
To compensate for this disruption in proprioceptive input, your brain does something called sensory reweighting. It shifts its cognitive processing resources from your proprioceptive system to a more reliable input such as your visual system.
After a musculoskeletal injury, such as an ACL tear in the knee, individuals have an increased reliance on vision for postural control.2 Unfortunately, in many rehabilitation programs, individuals are taught to rely on vision and an internal focus on where their limb is while performing an exercise, adding to this dysfunction. This can have implications when they return to sport, as the athlete must use an external focus strategy (focusing on opponents or a ball) and constantly integrate and react to their environment.
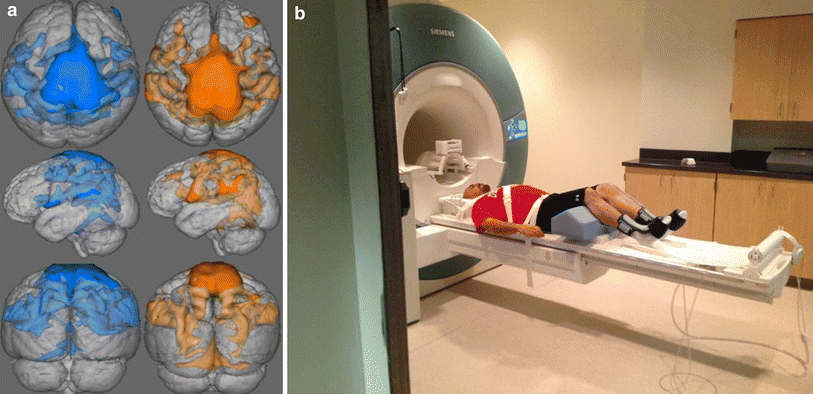
The problem with relying more heavily on vision is that there is an increased injury risk when participating in sports. Some motor regions in the frontal lobe are recruited as part of the brain’s sensory reweighting process after injury. As a result, the frontal lobe requires more cognitive resources and has less capacity to process other demands of sport, such as following an opponent’s ball or landing safely from a jump.2 Typically, experts at a physical skill show more efficient motor control firing patterns within the brain compared with novices. It’s concerning that an injury, even in elite athletes, can worsen the efficiency of this neural activation. These changes in the brain have been confirmed on fMRI and EEG studies, from two years after injury and up to five years after ACL reconstruction (ACL-R) surgery.3
To summarize, the two major changes in the brain after an injury are:
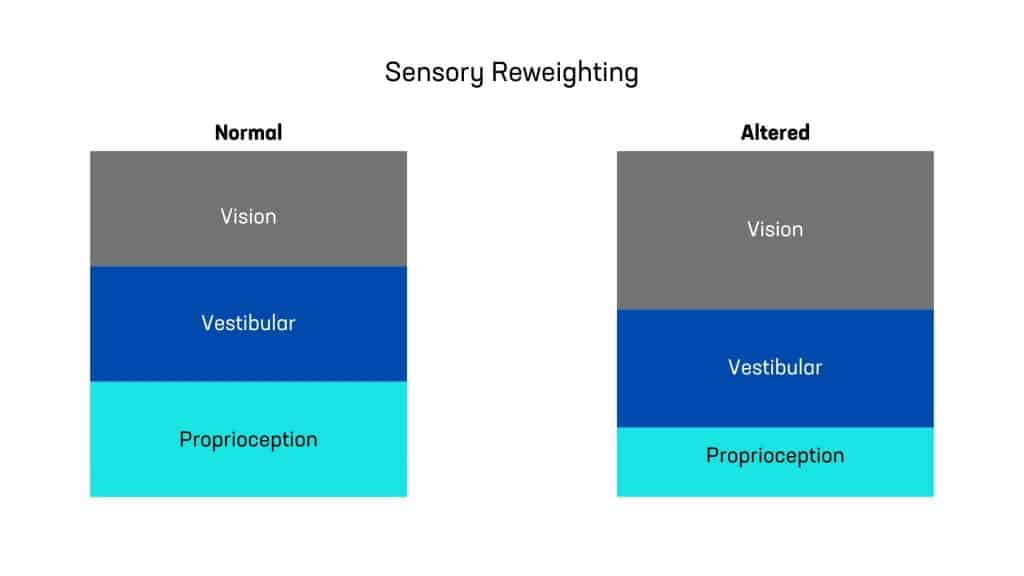
The goal of sensory reweighting therapy is to harness the neuroplasticity of the brain to shift the reliance from vision, as a strategy for body control movement tasks, back to the sensory signals from the joint and ligament receptors. One method that is gaining popularity is stroboscopic visual training (SVT) using specialty eyewear.
Stroboscopic glasses are a more precise method to control the amount of visual occlusion. Stroboscopic glasses recreate the visual, attentional, and neurocognitive demands of sport, within a controlled clinical environment. They do this by alternating between transparent and opaque lenses. These transitions can happen anywhere from 25 to 900 msec.2 By periodically blocking vision, the brain begins to upregulate the signals from other areas of the body – particularly the proprioception system. This training also improves visuomotor processing efficiency.
So far, studies have applied SVT to three main areas of rehabilitation – ankle sprains, knee injuries and concussion. The neurocognitive changes likely happen in most musculoskeletal injuries, but the research is new and has not yet been explored in other conditions.
While this is beyond the scope of this article, there are two main mechanisms by which stroboscopic training can improve performance.
Sports performance relies on quick decision-making, reaction time, attention to external events, and more. In fact, the superhuman-like ability for some elite athletes to “slow the game down” is thought to be due to enhanced reaction time.5 SVT helps shift attention from an internal to an external focus. External attention is superior to internal attention for sports performance and motor learning.4 The increased effort that is involved when using stroboscopic glasses helps once the glasses are removed. Athletes report that tasks feel easier and objects move slower. SVT also helps an individuals process visual information faster, giving them more time to perform appropriate injury-prevention movement strategies during a competitive game.7

One study tested the performance of professional ice hockey players before and after a 16-day preseason that included a protocol of using stroboscopic glasses. The group that trained daily with the strobe glasses showed an 18% improvement in their shooting precision compared to the control group.7 Although this was a small sample size, other studies have confirmed a significant improvement in athletic performance.
The current research has a wide range of training parameters. SVT sessions to improve performance can last anywhere from 5 minutes to 45 minutes with the glasses on.4 For rehabilitation, a protocol of 3 times per week of 20-minute sessions showed improvement in ankle stability.8 Like with many exercises that target the brain, it takes frequent repetition to elicit neuroplastic changes.
Unfortunately, the frequency needed for long-lasting results may be difficult for some people due to financial constraints. Thankfully, even a training session of 5-7 minutes can have an effect. To make this training tool more accessible for individuals going through rehabilitation, we have developed a membership program that gives daily access to our gym to use specialty equipment (including the Senaptec strobe eyewear).