
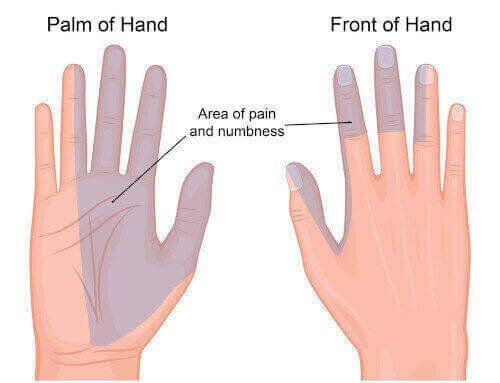
Carpal Tunnel Syndrome (CTS) is a condition that arises due to compression of the median nerve as it runs down the forearm and into the wrist. This compression typically results in pain, tingling and/or numbness in the palm, thumb, index, and middle finger and can extend into the forearm. CTS is the most common compressive neuropathy with a prevalence of 3-4%1.
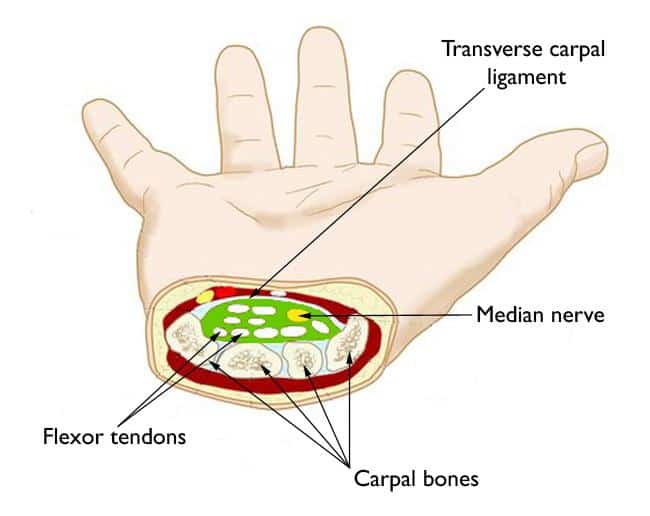
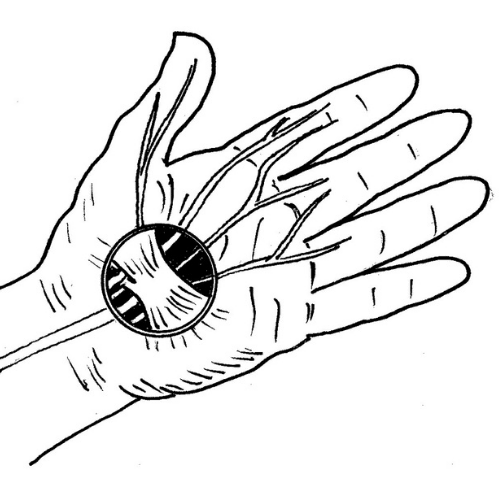
The carpal tunnel is an anatomical compartment located at the base of the palm which contains the median nerve as well as nine tendons of the hand and forearm. The boundaries of the carpal tunnel are formed by the bones of the wrist and the transverse carpal ligament. CTS results when there is a decrease in the size of the compartment, due to factors like overuse, trauma, or arthritis or an increase in the size of its contents due to swelling of the tissue around the flexor tendons, or both3. Since the walls of the carpal tunnel are non-extendable, built-up pressure is unable to escape and results in compression and irritation of the median nerve. This compression results in the hallmark weakness and altered sensation in the parts of the hand supplied by the median nerve.
Common risk factors for CTS include repetitive wrist movements such as typing or machine work, previous wrist injuries, pregnancy, diabetes, and autoimmune disease2.
CTS typically begins gradually with mild tingling or numbness, often at night or with sustained gripping of objects such as a phone or steering wheel. Patients often report feeling relief with stretching or shaking their hands4. As the condition progresses, feelings of tingling and numbness may occur more frequently and patients often complain of burning pain. Symptoms may eventually progress to muscle loss and decreased grip strength; which combined with sensory loss often results in complaints of weakness and often dropping things.
Individuals with CTS respond well to physiotherapy based treatment. Patients are advised to modify activities to include regular breaks, ensure proper hand ergonomics when typing, and decrease repetitive activities where possible5. Treatment usually involves manual therapy around the hand and wrist as well as exercise to relieve pressure in the wrist and improve blood flow to the irritated nerve. Progress can be monitored using a variety of tools, including handheld dynamometry to measure changes in grip strength.

Most current recommendations suggest activity modification as initial therapy rather than immobilizing braces. In some cases, it is recommended to wear a brace at night or during activities that are known to aggravate symptoms. However, a brace should not generally be used during the day as movement and use of the wrist are required to prevent muscle loss and stiffness7.
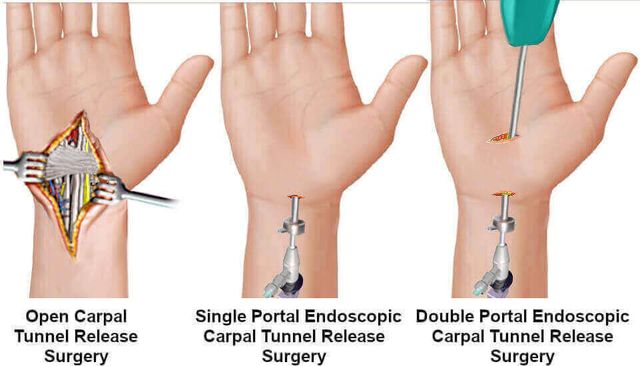
For more severe cases with unrelenting pain or in those who have persisting symptoms following conservative management, surgery to release the transverse carpal ligament may be recommended. Surgery was found to be most beneficial in the short term (6 months) to alleviate symptoms, however conservative management resulted in similar symptom relief in the long term (12-18 months).